Monaco 6®
面向放疗的高精度治疗计划
在近期发布的两个主要版本中,Monaco®迎来重大变革,对工作流程的效率和计划质量产生了立竿见影的影响。
从3D适形放疗到立体定向放疗,Monaco 6为各种治疗提供了简洁直观的计划功能,并整合了MOSAIQ®数据管理、自动计划和独特的质子计划功能。
Monaco® 6已在中国拿证,并拥有CE认证、美国 510(k)许可和加拿大医疗器械许可证。
简化日常工作流程
升级到Monaco可以节省大量时间

近期,在向Elekta Monaco治疗计划系统升级的过程中,GenesisCare 澳大利亚正在寻找一种可扩展、自动化且完全整合的解决方案,以部署到其分布在4000多公里范围内的37个放疗中心中。除了Monaco 6的自动计划功能提高了工作流程效率外,与MOSAIQ的整合还大幅降低了数据管理出错的风险。在短短几个月内,他们重新安排优化了工作流程,为计划人员节省了更多时间,使其能为重要的工作全力以赴:制定个性化的治疗计划和实施先进的技术。
将Monaco和 Elekta Harmony Pro 相结合的自适应治疗工作流程
借助快速的自适应计划工作流程,您将能够应对患者的变化。Monaco基于Elekta Unity先进的MR-Linac经验而构建,它整合了一套工具,用于执行触发式自适应工作流程。我们称之为反应引导放疗(RGRT)
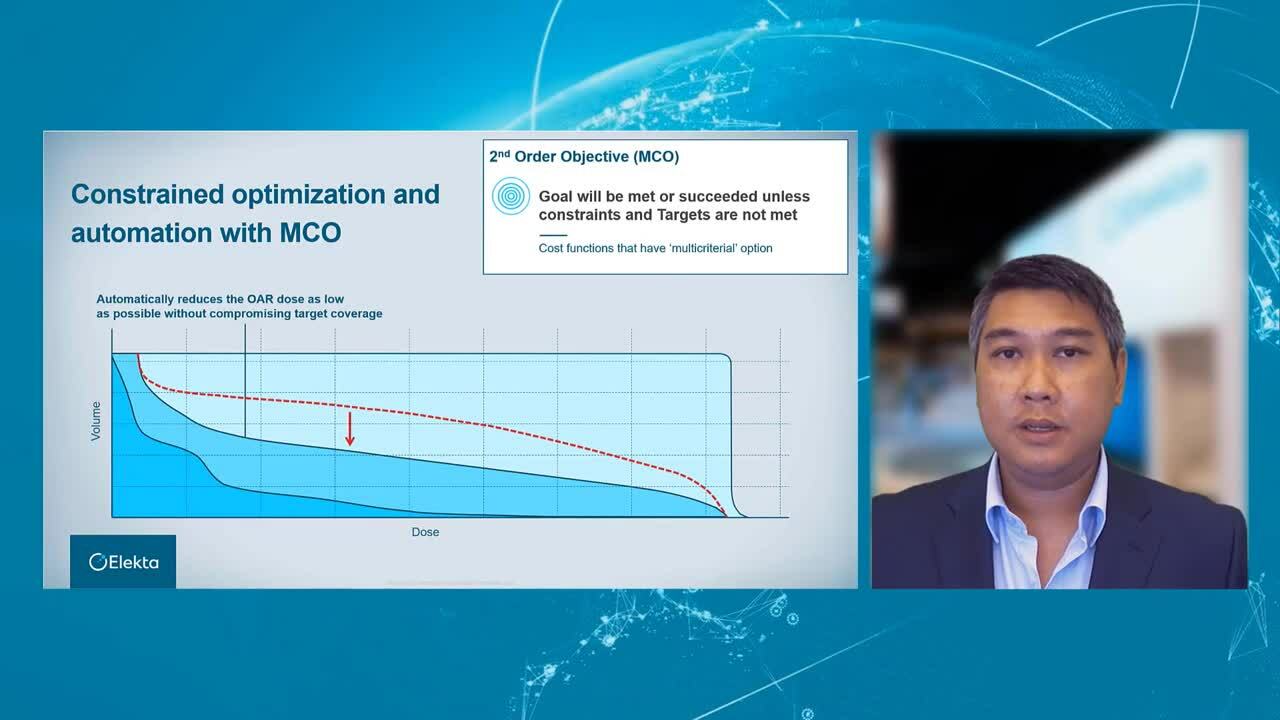
通过MCO实现您的临床目标
如何在最大限度地提高肿瘤照射剂量的同时,保护危及器官?如何尽量减少靶区和约束之间的权衡取舍?
Monaco独特的多标准优化(MCO)方法可以实时为您解决这些权衡取舍的难题。您不再需要探索所有可能的治疗方案。相反,Monaco会直接找到最符合您临床目标的计划。
具体请观看短视频。
IntelliMax为您的Monaco系统提供主动、个性化的支持"
Elekta IntelliMax®,人工智能(AI)领域的突破技术
- IntelliMax屡获殊荣,并且获益于最新的AI技术
- 超过75%的医科达预测性维护活动由人工智能算法生成,而且这一数字还在迅速增加
- 我们正在申请多项预测技术方面的专利
打破立体定向放疗的极限
提高SRS和SBRT治疗的可靠性、准确性和信心
了解Monaco和Versa HD如何帮助您制定高适形性SRS/SBRT 放疗的精确计划并实现高效执行。

亚毫米精度
完全集成的HexaPOD™ evo RT定位系统和IntelliBeam功能,增强了SRS的治疗信心。
一次治疗更多靶区
1毫米的虚拟叶片和完整的40 x 40厘米的射野尺寸,能够快速治疗多个非常小的立体定向靶区。
以更快的速度治疗更多患者
Versa HD具有HDRS功能,可让您在标准的15分钟或更短的时间内完成任何SRS/SBRT放疗。
高清动态放疗——探索医科达的优势
"Monaco在立体定向放疗方面具有多种优势。对于多发性脑转移瘤,我们使用Monaco,因为它充分发挥了Agility准直器的优势,特别是分割方面。对于肺部治疗,蒙特卡罗算法使我们有信心,确保剂量计算的准确性,即便是非常小的靶区,也不例外。"
Frank Lohr教授,意大利摩德纳综合医院肿瘤科放疗服务主任兼UniMORE放射肿瘤学住院医师项目主任。
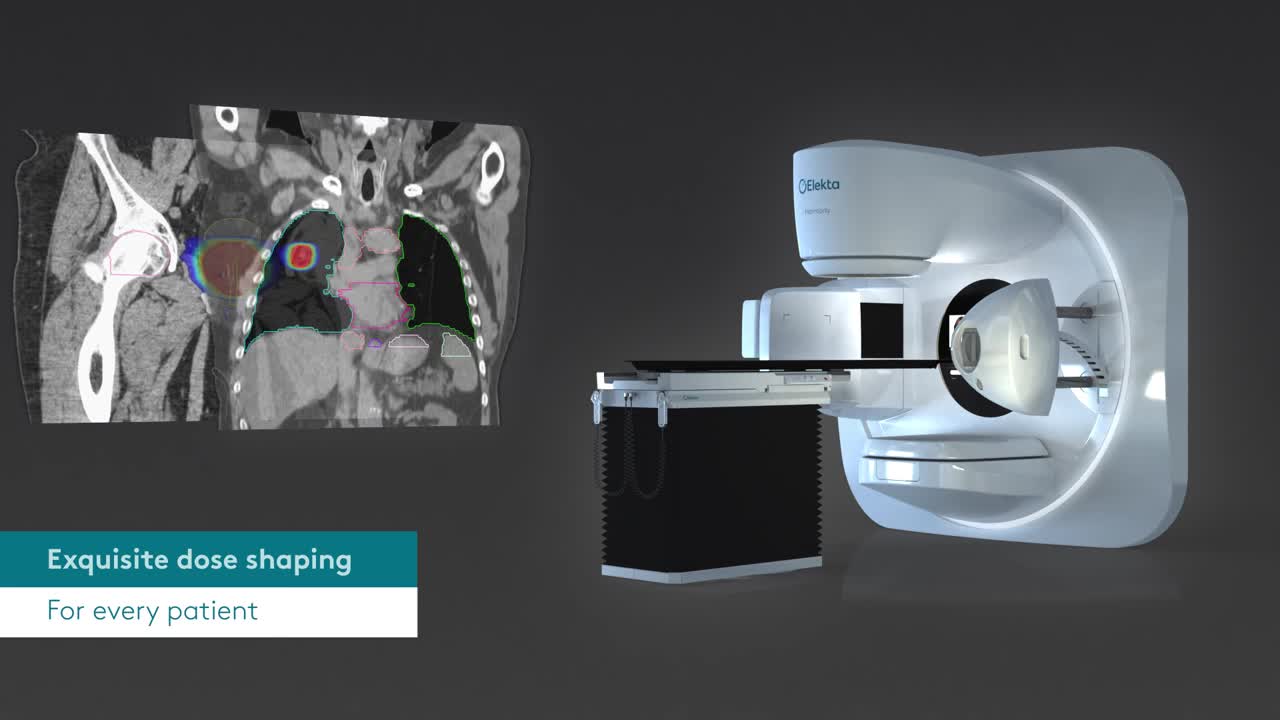
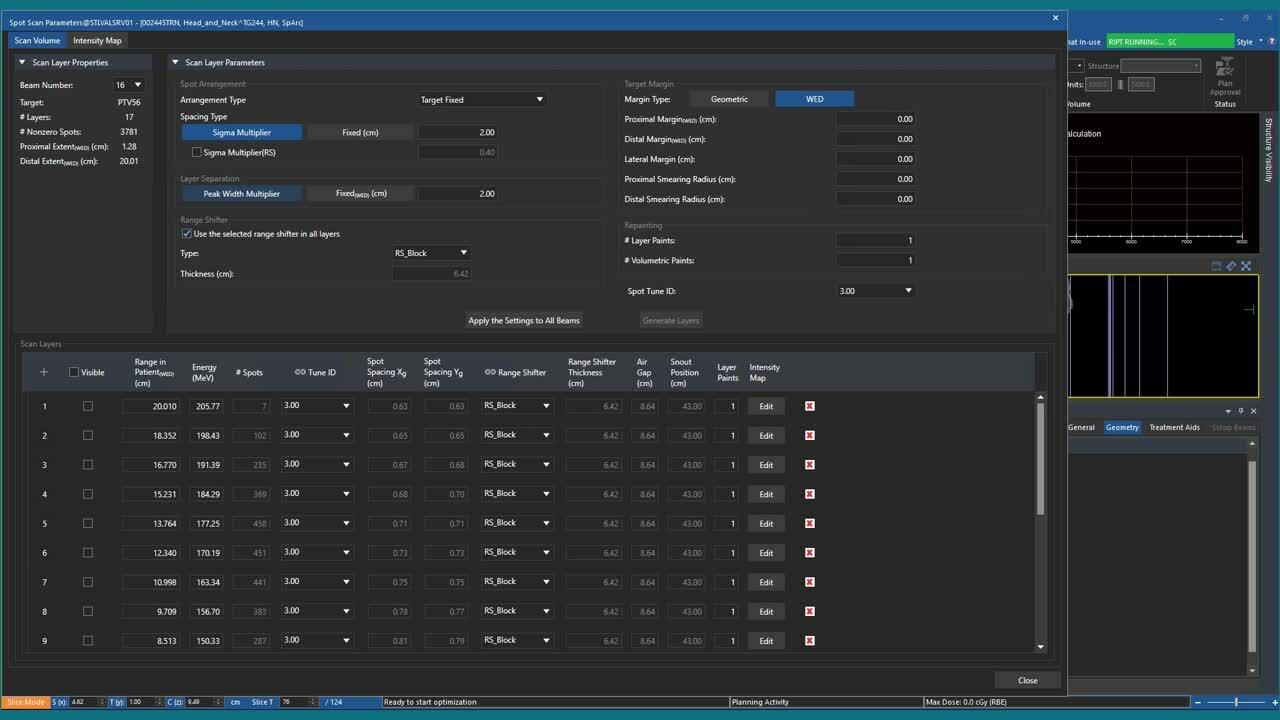
质子治疗软件的理想合作伙伴
Monaco 6推出的质子治疗的计划功能,扩展了计划功能,与MOSAIQ和Elekta ProKnow一起,提供一个完整的软件生态系统,并可管理任何光子或质子治疗。Monaco提供了专门用于高效斑点定位、自动射程器优化、LET评估和鲁棒优化的质子特定工具,以实现质子治疗的强大而简单的工作流程。
简单、优质、组合
医科达质子软件结合其精准放疗领域的数十载创新,以及治疗计划和自适应解决方案的丰富经验,专为时时刻刻满足患者旅程中的需求而设计。通过与IBA合作,医科达提供了一种全面解决方案,该解决方案与IBA ProteusONE和ProteusPLUS质子治疗系统完全集成。

通过质子弧形治疗改善患者的日常治疗

"我们确实发现,质子弧形治疗可能对更广泛的临床适应症具有潜在的临床益处。与传统的IMPT相比,所有剂量计划的质量都得到了显着改善"
Xuanfeng (Leo) Ding博士,美国密歇根州罗亚尔奥克William Beaumont Health System 质子束治疗首席医学物理学家
Interview with Dr. Xuanfeng (Leo) Ding, PhD, Lead Medical Physicist, Proton Beam Therapy, William Beaumont Health System, Royal Oak, Michigan, USA
Can you tell us a bit about who you are and what you do in Beaumont Proton Therapy center?
My name is Xuanfeng Ding, but you can call me Leo. I am the lead proton physicist at Beaumont Health. Clinical service is my primary job but I enjoy doing innovative research and teaching during my spare time.
How long have you been working in the field, and how have you seen Proton Therapy evolving in the past few years? What do you see as the most important trends in the coming years?
I have been working in the field of proton beam therapy for about ten years. This decade has seen a dramatic change in the landscape of the proton beam therapy market, from the technology side. We are moving from Passive-scattering, to PBS, and we're now developing the rotational proton arc therapy. It is just like the revolutionary era of LINAC development in the 1990s to 2000s where CBCT, IMRT and VMAT were invented and clinically implemented. That changed the entire landscape of photon radiation therapy. We are in the middle of the revolutionary development of proton beam therapy.
From my personal view, there are two main trends in proton beam therapy:
- Continuous development of the treatment/imaging technology aims to provide more robust, fast and accurate treatment for our patients.
- Further reduction of investment and operational costs of the proton system, so more proton centers can be introduced into our local community and more patients can access these advanced cancer treatment technologies within driving distance.
Why is Arc Therapy, specifically, important to implement for protons?
Excellent question. Arc therapy solves the three major challenges:
- Dose conformity. The current IMPT technique only uses a limited number of treatment fields, which may not provide an optimal treatment plan quality. People may ask, why not deliver more beam angles? Yes, we could, but the delivery efficiency is slow using proton, and the proton center cannot afford that beam time. So, the proton arc opens up the degree of freedom to the arc trajectory to optimize a better and faster treatment plan.
- Treatment efficiency. It simplifies the clinical treatment workflow compared to the conventional IMPT, which effectively improves the treatment throughput of a proton center. It could increase the revenue of the proton center and more patients could be treated in each proton beam therapy facility.
- It provides a more robust treatment dose against a lot of uncertainties that were the weakness of conventional proton beam therapy. More recently, we published a series of papers on the lung cancer SBRT and Spine Mets SBRT that showed a tremendous improvement in robustness.
Why has this not already been done?
First, I think it's because of technology limitations. A proton gantry normally weighs hundreds of tons. To deliver a proton spot in a submillimeter accuracy while rotating such a giant machine is a big engineering challenge. Not too many people thought about this crazy idea at that time.
Second is the energy layer switching system. The technique was not matured at that time, which cost several seconds to switch each energy layer. As a result, to deliver an arc plan with hundreds of energy layers 10 years ago would cost half an hour or more. It was just not feasible to implement it in clinical routine, so there was no market at that time.
The third issue was that there was no one treatment planning system on the market 10 years ago that was able to generate such complicated proton arc plans. As a result, no one had demonstrated that such a concept was compatible with the existing clinical proton system, and no one had conducted a series of comprehensive study to demonstrate the potential clinical benefits utilizing proton arc therapy.
About 6 years ago, our team—Dr. Li and I were still very young and very naïve at that time—believed in this concept. So, we worked day and night to solve this problem, and the result is promising and exciting. Our proton vendor, IBA, believed in us and collaborated with us on this crazy project. And now, it works—we delivered the first prototype proton arc therapy using a clinical system at Beaumont in 2018. This is one of the milestones that changed people's minds that arc therapy is not a concept anymore. It has become reality.
Intuitively, Proton Arc seems to be linked to an increased dose bath. Is this not against what proton therapy is trying to achieve?
Yes or no. It depends on how you define the dose bath.
Compared to the conventional IMPT, we found that Arc therapy can reduce about 10% of the patient's body integral dose in different disease sites because of its better conformity, and because it's optimized for a shorter beam path.
Low dose bath—e.g., 0.5Gy or 1Gy volume—will be higher than IMPT. Such a low dose bath could be very important to our pediatric patient population, where the chance of secondary malignancy may increase. Still, proton arc is much better that VMAT. In these clinical situations, clinical users can use partial arc therapy instead of a full arc. So, it offers the equivalent dose distribution compared to IMPT.
I am not saying Arc therapy is going to replace everything. This is a just new treatment platform; the user can use it wisely to benefit the patients who need this technology.
Does Proton Arc Therapy improve the robustness of treatment plans?
Yes. With the degree of freedom through the arc trajectory, we demonstrated the improved plan robustness in multiple disease sites through a series of publications, e.g., lung mobile treatment, which mitigates the breathing-induced motion interplay effect and, e.g., spine mets SBRT, which showed proton arc can mitigate dose perturbation in situations where the patient geometry changes. So, degree of freedom matters a lot in proton beam therapy. People may not like the low dose bath, but it helps in the treatment robustness.
How does Proton Arc impact patient throughputs?
Proton arc therapy improves the daily patient treatment throughput based on three mechanisms:
- Reduce the number of isocenters. If the patient's tumor or target is large—for example, the chest wall or breast, which requires two iso to cover the entire target—SPArc can irradiate the entire target through one iso. Saving one iso means reducing about five minutes from the couch movement and imaging validation process.
- Simplify the treatment workflow. Normally therapists need to rotate the gantry to the extract gantry angle and then request the proton beam. With proton arc, our therapists only need to request once, and treatment delivery is automatic, and the gantry rotates automatically. This simplification saves a lot of time in the clinic. Based on statistics from our own proton center, an IBA single-room system, we are expected to treat 20-25% more patients per day. I think it would work even better for a multi-room system.
- Treatment of mobile tumor using repainting technique may take a lot of time using IMPT SBRT. SPArc therapy could provide the same level of robust target coverage as volumetric repainting, which we published this year on lung SBRT.
What would be the best indications for Proton Arc, and why?
I don't think I am able to give you or the community a definitive answer today. We are still in the preliminary investigation stage.
However, based on the current studies that we published, we did find a lot of potential clinical benefits for a broader range of clinical indications such as non-small cell lung cancer, head & neck cancers, brain tumors, prostate cancer, etc. All the dosimetric plan qualities are significantly improved compared to conventional IMPT.
Whether or not such dosimetric quality improvement will translate into better clinical outcome, we don't know at this moment. But I am pretty confident it will do so, just like IMRT to 3D conformal. So, let's first make Arc therapy clinically available to our patients.
One thing I need to mention is that our radiation oncology society is moving towards the hypo fractionated treatment, conventional IMPT was not widely considered as an SBRT/SRS treatment option for a lot of reasons—for example, the inferior dose conformity and more sensitivity to the uncertainties. But I think SPArc technique will change this paradigm. It could become a new standard treatment option for SBRT/SRS. especially in the era of concurrent chem-RT or immo-RT. So, this new technology will help proton market expand its clinical indication and benefit more patients in the hypofractionation regimen.
How can Elekta help you bring this new technology to the market?
[Elekta can] definitely [help]. As I mentioned before, there are two main ongoing aspects of development:
- One is the proton beam therapy system itself, which allows us to dynamically rotate the gantry while delivering the proton radiation. In this direction, we are collaborating with IBA, our proton manufacturer.
- The second one is the treatment planning system to support this advanced treatment modality. TPS has played a key role in radiation therapy for decades. Without a TPS vendor, there is no way we could implement such a nice technique into routine clinical practice. I've used Elekta's Monaco [treatment planning system] since I was a graduate student in photon radiotherapy 15 years ago. And I am glad to see Monaco now entering the proton world with an FDA-cleared clinical solution. With all the expertise and developers, the collaboration between Elekta and our clinical team will lead to a better, more efficient proton arc optimization platform, which is critical to a faster adoption of this new technology in our community and will benefit more cancer patients.
质子治疗的未来。现在,人人皆可。
一款综合性软件解决方案
在医科达,合作至关重要。美国什里夫波特Willis-Knighton医疗中心是一家历史悠久的放疗中心,其团队一直在使用医科达直线加速器和IBA质子治疗设备。在此,他们分享了有关使用我们的最新解决方案的体验,以及IBA和医科达合作的相关体验。
"可视化工具与约束表的反馈相结合,可以帮助您更好地进行优化,因为所有信息都唾手可得。"
Kuan Ling Chen博士,美国什里夫波特Willis-Knighton医疗中心。
改进质子治疗计划
位于捷克布拉格的捷克质子治疗中心,是世界领先的质子治疗提供商之一,自2012年营业以来,已经治疗了5500多位患者。该中心拥有4间治疗室,均配备了IBA技术、医科达治疗计划和肿瘤信息管理软件。快来阅读更多信息,了解其使用Monaco质子解决方案的经验。
"基于GPU的蒙特卡罗剂量计算算法的速度确保我们能够快速制定计划,而且我们得到的计划质量非常出众。"
Vladimir Vondráček,捷克布拉格,捷克质子治疗中心医学物理部主任。
Read more in FOCUS